


Introduction:
Priapism is a persistent penile erection not associated with sexual stimulation lasting for more than 4 hours. It is seen in up to 1.9% of patients with CML in some centers. Priapism adversely affects the quality of life, sexual function, of the affected patients. Long-lasting priapism is associated with a drastic effect on male fertility. The underlying pathophysiology involves disturbed autoregulation of the penile circulation through nitrous oxide (NO) and phosphodiesterase enzyme dysregulation.
Method
Literature searched in google scholar, PubMed, and Scopus search engines with keywords priapism, chronic myeloid leukemia, chronic granulocytic leukemia, and chronic myelogenous leukemia (English literature between 1960 to 2020)
Results
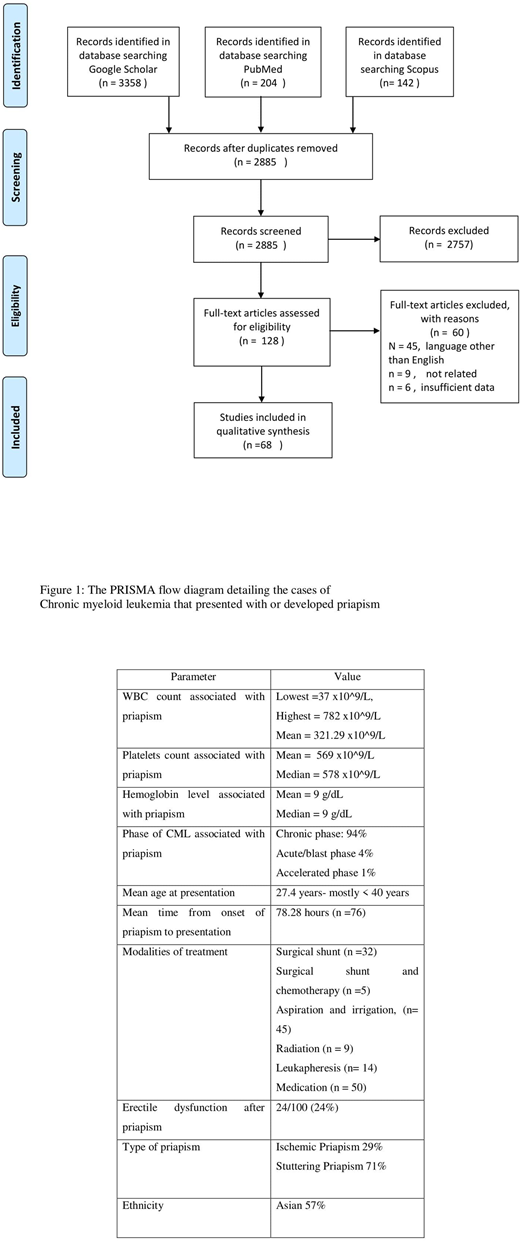
One hundred cases of priapism were reported in patients with CML. Most patients were below the age of 40 with mean 27.4years. The youngest was 7 weeks old and the oldest was 60 years old. Most patients had priapism as the first presentation of CM, 3 developed priapism after starting the treatment, 2 after stopping treatment, one noncompliant with treatment,1 previously diagnosed, and 1 patient post-splenectomy. The majority of patients' priapism occurred during the chronic phase of the disease and only 5/100 had priapism during the blast and accelerated phase. They had a mean WBC = 321.29 × 109/ (n=92), and mean platelet count = 569,000 (n=69). The lowest WBC count associated with priapism was 37 x10^9/L, the highest was 782 x10^9/L. Treatment modalities included medications, aspiration and irrigation of the corpora cavernosa, radiation to the penis, leukoreduction, and surgical shunts. Medications were used in (N = 50), aspiration of the corpora cavernosa in (N = 45) patients, leukapheresis in (N = 14), radiotherapy in (N= 9), and shunt in (N = 32). Surgical shunt relieved priapism in (N = 16), another 5 had shunt with partial response and needed chemotherapy to control the priapism. 19 patients responded to aspiration and irrigation, and another 2 required chemotherapy to control priapism. Radiation was helpful in resolving the priapism in 3 patients and Leukapheresis was useful in 5 patients. Medications alone were used to terminate priapism in 10 patients, however, priapism persisted for a longer duration compared to other modalities.
It has been known that priapism lasting > 24 hours poses a high risk of permanent erectile dysfunction (94% or more). In 76 of CML patients with priapism, the mean time from onset to the presentation was 78.28 hours (three times longer than the high-risk period). The erectile function was affected in 24/100, not affected in 15/100, and not addressed in 61/100.
Conclusion:
Although priapism is an uncommon complication of CML, its fast diagnosis and management is crucial to avoid permanent erectile dysfunction.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal